INTRODUCTION
Scleroderma-is a spectrum of related disorders characterized by skin thickening from excess of collagen fibers and by abnormalities in immune, endothelial and fibroblast cell function.
LeRoy, EC, Black, CM, Fleischmajer, R, et al. Scleroderma (systemic sclerosis): Classification, subsets and pathogenesis. J Rheumatol 1988; 15:202.
BASIC ANATOMY OF THE SKIN

Source: Wikipedia, the free encyclopedia
The skin(cutis) and subcutaneous tissue contain arteries, veins, capillaries, lymphatics, hair follicles, sweat glands, sensory nerve endings,autonomic nerves, smooth muscles, fibrous connective tissue and elements of the immune system, all of which can be affected by scleroderma.
CLASSIFICATION
Scleroderma is a subset of systemic sclerosis involving the skin. A universally acceptable classification is still developing. The four categories listed below are clinically useful.
Diffuse cutaneous systemic sclerosis (dcSSc)
Limited cutaneous systemic sclerosis (lcSSc)
Systemic sclerosis sine scleroderma (patients with only internal organ involvement)
Environmentally-induced scleroderma (a probable cause of scleroderma in this case report)
DIAGNOSTIC CRITERIA FOR SCLERODERMA
Incidence: 4 to 12 cases /million/year
Female to male ratio of 4:1
Peak age: 30 to 50 years
Distribution: World wide
Clinical Presentation:
Skin: taut, red with loss of creases and hair, decreased movement of the skin
Raynaud phenomenon-a vascular spasm of small blood vessels leading to discoloration of fingers or toes due to temperature changes (cold or hot) or emotional events)
 Source: Wikipedia, the free encyclopedia
Source: Wikipedia, the free encyclopedia
Musculoskeletal System: arthritis (joint inflammation), myopathy (neuromuscular disorder due to muscle dysfunction)
Gastrointestinal tact: Esophageal and gastrointestinal dysmotility (difficult movement of the stomach and small intestine), dysphagia (difficulty swallowing) and gastroesophageal reflux of stomach acidic contents into the esophagus (GERD)
 Source: Wikipedia, the free encyclopedia
Source: Wikipedia, the free encyclopedia
Narrowing of the esophagus due to scaring from long term acid reflux from the stomach
Lungs: Alveolitis, pulmonary fibrosis, pulmonary hypertension
 Source: Wikipedia, the free encyclopedia
Source: Wikipedia, the free encyclopedia
Pulmonary Fibrosis
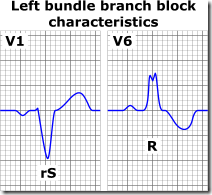
Heart: Myocardial fibrosis. White areas in the heart muscle (left); in the septum (right) He has a Left Bundle Branch Block as an effect of fibrosis in his septum
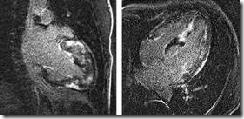 Source: Tex Heart Inst J. 2002; 29(3): 176–180
Source: Tex Heart Inst J. 2002; 29(3): 176–180
 Source: Wikipedia, the free encyclopedia
Source: Wikipedia, the free encyclopedia
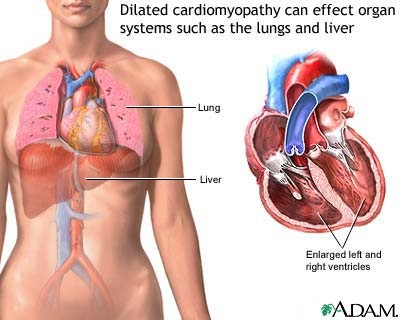
Dilated Cardiomyopathy
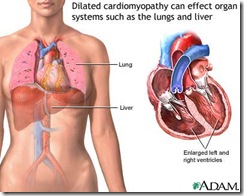 Source: Medline Plus
Source: Medline Plus
Kidney: Renal failure, hypertension
Thyroid: Hypothyroidism
Genitalia: Erectile dysfunction
Nerves: Entrapment Neuropathy e.g. Carpal Tunnel Syndrome and others
Etiology: Unknown.
Possible causes: connective tissue activation, immune abnormalities, inflammation and vasoconstriction
Laboratory:
Antinuclear antibody, Rheumatoid Factor; Anti-centromere antibody; specific organ abnormalities
Technical Studies:
Gastrointestinal tract: Barium swallow, cine esophagography (motility video), endoscopy, esophageal manometry (pressure changes in the esophagus during swallowing)
Lungs: Chest X-ray, Pulmonary function studies, CT scan of the chest, bronchoscopy with biopsy. Gallium lung scan, broncho-alveolar lavage (washings)
Heart: ECG, ambulatory ECG, echocardiography, cardiac catheterization
Kidney: Renal biopsy
Skin: Skin biopsy
Treatment:
General: D-penicillamine, recombinant relaxin, cyclophosphamide, methotrexate (UpToDate January 2008)
Raynaud phenomenon-(vascular spasm of small blood vessels leading to discoloration of fingers or toes due to temperature changes (cold or hot) or emotional events):
Calcium channel blockers (Varapamil), peripheral alpha-adrenergic blockers (Minipress; Cardura)
Arthralgia: NSAID’s (non-steroidal anti-inflammatory drugs)
Skin: moisturizing agents
Esophageal reflux: H-2 receptor blockers-reduce gastric acid ( Cimetedine, Tagamet, Zantac), proton pump inhibitors (Nexium)
Lung: Oxygen, lung transplantation
Kidney: ACE inhibitor (Captopril), dialysis, and kidney transplant
REFERENCES:
Siebold JR: Scleroderma. In Kelley WN et al (eds): Textbook of Rheumatology ed 5
Philadelphia 1997 WB Saunders.
Wachtel, Tom J author, Ferri’s Clinical Advisor p.633, 2002 Edition, St. Louis.
MEDICAL PROFILE OF THE CASE
FIRST ITERATION
7/9/02
HISTORY: A 61 year-old white male with a history of Scleroderma since 1989. Arthritis developed three years ago. He has the Raynaud phenomenon, ulcers of his fingers, slightly altered renal and cardiac function with a small pleural and pericardial effusion. Mild hypertension is controlled with Calcium/Magnesium tablets and with 10 mg of Quinapril, an ACE (angiotensinconverting enzyme) inhibitor and is taking thyroid hormone replacement for hypothyroidism. He has erectile dysfunction.
PAST HISTORY: The patient was an avid outdoors-man during his teenage years into his 20s. He collected snakes for research purposes and as a result had several envenomizations. He has had numerous tick bites and one Brown Recluse spider bite. It was the patient’s opinion that Scleroderma symptoms started shortly after "allergy?" injections. Besides living near the Great Dismal Swamp in southeastern Virginia, he lived in Panama and Southeast Asia and traveled into the interior parts of the Mexican jungle.
TREATMENT: Intravenous EDTA chelation and antioxidant nutrients. He refused Penicillamine, Methotrexate and Prednisone.
PHYSICAL EXAMINATION: A well-developed white male with shiny, taut skin of his face and extremities, atrophy of the skin of the fingers with Raynaud’s phenomenon, ulceration of the tip of the right middle finger, stiff joints of the hands and feet and muscle atrophy. HEART: normal. LUNGS: normal.
PROFILE DEVELOPMENT AND REPORTING
For research purposes I changed some of the names used in electrodermal screening. This newer technology reflects an upgrade of the acupuncture model because it includes electromagnetic analysis of both energy and information, not just energy alone.
Instead of electro-acupuncture, I use Electrodermal Detection since I do not produce a current of injury by puncturing. I apply a probe that closes an electical loop that includes information in the subject and information in the computer.
Instead of control measurement point (CMP), I use Main Detection Site. CMP is derived from KMP (kontrol mess punkt) a German acupuncture term.
Instead of acupuncture point, I use Electrodermal Detection Site. I do not insert a needle at a specific skin point. I apply a positive electric probe at a specific skin site for the purpose of detecting an electromagnetic signal at that site.
Instead of acupuncture meridian, I use Detection Array because it defines a set order of linear signals in the context of an electromagnetic model.
The electrodermal profile was obtained by testing the Main Detection Sites for each Detection Array and then testing each Detection Site on the array, only if the main detection site was abnormal. At times detection sites were chosen based the site of a clinical condition alone. I have a list of detection sites arranged according to organs and systems and a graphic display of all the detection sites in my book An Electrodermal Analysis of Biological Conductance.
In this report I listed organs, systems, clinical conditions and assessment of each iteration in BOLD CAPITAL letters.
Each detection site has:
A capitalized bold letter/number combination
An abbreviation of a detection site e.g. SV 48– Secondary Vessel 48 a site on the mid palm proximal (toward the body) of the ring finger
A real language name for the site(s) of origin of a code e.g. striated muscle.
A frequency from a frequency generator. Each "X" equals 50-60 cycles per second.
A cognitively derived value of the time that a signal became detectable
ELECTRODERMAL PROFILE OF THE CASE
MUSCULOSKELETAL SYSTEM
SV 48 Striated Muscle: Borrelia burgdorferi ; 8X; Time: 53 years
SV 47 Smooth Muscle: Borrelia burgdorferi; 8X
HT 6 Myocardium: Borrelia burgdorferi; 8X
CI 4a Muscular Layer of the Arteries: Borrelia burgdorferi; 8X
CIRCULATION
OR 1c-1 Microcirculation of Degeneration: Transforming Growth Factor 3X; Beta Glucan 3X; Feline Infectious Peritonitis virus 3X
SMALL INTESTINE
SI 1b Small Intestine, Main Detection Site: Candida rugosa 3X; DDT 3X; Time-46 years
ERECTILE DYSFUNCTION
BL 33 Sympathetic Nerve (Pelvic Portion): Candida rugosa 3X
AL 1a Autonomic Nerve allergy: Leishmania mexicana mexicana 3X; Time: 38 years
SKIN RASH, FACE
SK 3 Skin of the Head: Pyrogenium Suis (Pork); 4X; Time: 97 years
ASSESSMENT
Borrelia burgdorferi was the most frequent signal in this case initially.
Sites with a signal for Borrelia burgdorferi:
SV 48 Striated Muscle sites
SV 47 Smooth muscle
HT 6 Myocardium
CI 4a Muscular wall of arteries
The Borrelia burgdorferi signal was imprinted in his biofield 58 years ago when he was 8-years old. He lived in a town adjacent to the Great Dismal Swamp in southeastern Virginia, an area where there is a heavy deer and tick population. Borrelia signals were detected at smooth muscle and striated muscle sites. The smooth muscle of the esophagus are associated with dysphagia (difficulty swallowing) and smooth muscles of the arterial wall relate to the skin ulcer of his right middle finger, atrophy of the skin, ischemia and the Raynaud phenomenon. Muscle atrophy could be related to Borreliosis. (Rheumatology (Oxford) 2005 May;44(5):587-96).The Muscular Layer of the Arteries site, CI4a at which the Borrelia burgdorferi signal was detected may be associated with tissue ischemia. (Rheum Dis Clin North Am 2003 May;29(2):275-91)
The Microcirculation of Degeneration Site OR 1c-1 seems be an important site for detection for Scleroderma. Transforming Growth Factor, a cytokine; Beta Glucan a biological defense modifier; and Feline Infectious Peritonitis virus , an animal virus were identified at this detection site. Feline Infectious Peritonitis virus produces intense inflammation in cats. It is an example of an animal virus signal identified in a human subject. It not unreasonable to suspect an inflammatory reaction in the human host as well. (NEJM Volume 342:1350-1358 May 4, 2000 Number 18).
The detection of a signal for Feline Infectious Peritonitis virus in a human subject electromagnetically indicates that this virus usually found in animals can also be detected in humans.
The electromagnetic signal for Transforming Growth Factor was detected. TGF-beta is a cytokine involved in pulmonary fibrosis. This finding is important since it opens the possibility for investigating cytokine activity in the pathogenesis of disease by using an electromagnetic model.
Other important non-coherent conductance signals are from Candida rugosa and DDT. Candida rugosa is an emerging pathogen (Journal of Clinical Microbiology, October 2006, p. 3578-3582, Vol. 44, No. 10).
The DDT, a pesticide signal, has been biologically imprinted in his body water for 48 years, ever since he was 13 years old. At that time his father used DDT as a pesticide on his farm. DDT has a 30 year biological half-life.
The date of the imprinting the signal for Candida rugosa in the electromagnetic matrix is more difficult to reconcile since it’s time of entry was determined to be 4171 years ago. If the cognitive method of dating time of detectability of a non-coherent conductance wave is valid, then, 4171 years is a process that began modifying electromagnetic structure a long time ago in his progenitors and is not one that had been acquired within his lifetime.
It has been my experience that DDT and Candida species are frequently identified together at the Small Intestine Detection Site, SI 1b and pose the possibility that there is a cause and effect relationship between the two. It is rare to detect Candida species without also detecting DDT at the same intestinal site. In this case the signal for Canada rugosa and DDT are detected at the Small Intestine Detection Site SI 1b.
Canada rugosa stands alone at the Pelvic Portion of the Sympathetic Nervous System Site, BL 32. I have observed that the signals for Candida species are frequently detected at at Sympathetic Nerve detection sites. The Candida rugosa wave has caused a destructive interference at the detection site for the Pelvic Portion of the Sympathetic Nerve and indicating an electromagnetic relationship with his erectile dysfunction.
Leishmania mexicana mexicana was found at the Autonomic Nerve allergy AL 1a. Leishmania mexicana mexicana is a hemoflagellate protozoan from Mexico, Guatemala, and Belise causing New World cutaneous leishmaniasis called chiclero’s ulcer, a single ulcerous lesion. The New World sandfly, Lutzomyia olmeca is the vector.
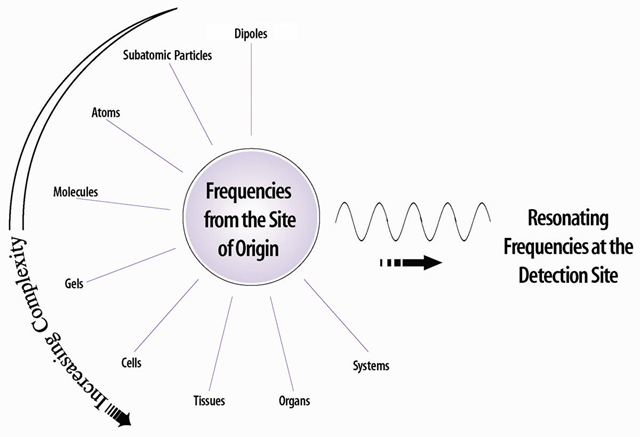
COMPLEXITY OF THE CONDUCTDED SIGNAL
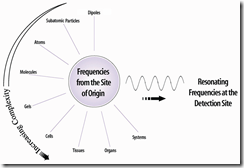
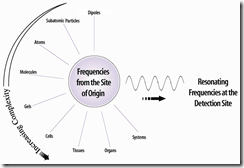
The conductance wave is very complex. It is made up of all of the coherent and non-coherent waves coming from a common site of origin. Destructive and constructive interference of these waves results in the formation of a conducted wave that radiates to a site on the skin through the bodies extracellular matrix, interacting with numerous electromagnetic fields along the way, eventually reaching detection sites on the skin through fairly well established electromagnetic channels. From an electromagnetic perspective, the electromagnetic fields in the sol-gel-electrolyte extracellular matrix make an electromagnetic matrix or an electromagnetic structure through which energy and information flow.
If there is no change in skin resistance at a detection site, then the conducted wave is considered normal. This means that all of the waves arising from the Site of Origin are coherent.
A change in skin resistance indicates that there is an abnormality in one or more of the components of the waves that radiate in the conductance pathway. The result is a non-coherent conductance wave that results in a change in galvanic skin resistance and a drop in the reading of the ohm-meter.
SECOND ITERATION
9/30/02
INTERVAL HISTORY: Patient states that he feels worse, short of breath with abdominal tightness and fatigue.
ELECTRODERMAL PROFILE
(Electromagnetic site designation; Plain language nameof the site; Signal in plain language; Frequency; Time in the biological field
MUSCULOSKELETAL SYSTEM
SV 48 Skeletal Muscle: Borrelia venezuelensis 32X
SV 47 Smooth Muscle: Pneumocystis carinii 3X T: 15 years
FIBROUS CONNECTIVE TISSUE
FI1b Connective Tissue:
Tetracaine 4X
Influenza Vaccine 1993-99 3X
Swine Flu Vaccine 3X T: 30 years
Ornidazole 3X
Toxocara mystax 3X
Dermanyssus pteronyssinus (house dust mite) 3X
Timeresurus elegans 3X T: 24 years
Loxosceles reclusa 3X (Brown Recluse Spider)
SKIN
SK 1-4 Lymphatics of the Subcutaneous Fascia:
Swine Flu Vaccine 3X
Loxosceles reclusa 3X
JOINTS
LI16 Finger Joints:
Swine Flu Vaccine 3X
Loxosceles reclusa 3X
ASSESSMENT
Borrelia venezuelensis– a new signal depicting a species change that has taken place in the Borrelia genus at the Skeletal Muscle Site SV 48. This change may be related to the polythetic nature of Borrelia reacting to a change in an internal electromagnetic environment from the signal induced solution of Borrelia burgdorferi, previously given. The resonance has increased from 3X to 32 X (From 150-180 cycles per second to 1600 cycles per second to 1920 cycles per second)
Dermanyssus pteronyssinus 3X-an Acaris house dust mite, affecting the Connective Tissue Site FI 1b.
Influenza Vaccine 1993-99 3X-a vaccine used for influenza prophylaxis still resonates after 30 years in the Connective Tissue Site FI 1b; Lymphatics of the Subcutaneous Fascia SK 1-4 and Finger Joints LI16 .
Loxosceles reclusa 3X- the Brown Recluse Spider
Ormidizo 3X-an anti-protozoal drug.
Pneumocystis carinii 3X- a latent yeast form activated in an immune compromised state is detected after 15 years at the Smooth Muscle Site SV 47.
Tetracaine- a dental anesthesia is detected in the Connective tissue site FI 1b. He has had a history of local dental anesthesia with a "caine"
Toxocara mystax: a common round worm of cat’s that is transmitted to kittens by eggs. In the kitten’s intestine the eggs release second-stage larvae that migrate to the heart, lungs trachea and gut.
Timeresurus elegans is a green colored pit viper of Eastern and Southeast Asia. A destructive interference signal for T. elegans has been present for 24 years. The subject does not recall having been bitten by T. elegans but has been bitten numerous times by another pit viper, the copperhead or Agkistrodon contortrix, common in the Great Dismal Swamp. There may be a portion of the Copperhead pit viper venom signal that is common electromagnetically with the signal of T. elegans venom making the signal less specific than the name would indicate. Sensitivity and specificity studies are needed to clarify this issue along with a sequence analysis of the pulse code of T. elegans encrypted in the computer.
PLAN: Continue the iterative process and look for change in SV47/SV48/FI1b/Ski-1/LI 16 and other detection sites.
THIRD ITERATION
12/5/02
INTERVAL HISTORY: He has observed a gradual toward improvement since his last iteration. Only during the winter did his Raynaud’s symptoms get worse, however, the atrophic skin ulcers have begun to heal. Skin tightness remained the same. Sleep disturbance, spaciness, abdominal bloating and gastro-esophageal reflux all responded completely. His musculo-skeletal complaints remained about the same.
ELECTRODERMAL PROFILE
(Electromagnetic site; Plain language name; Signal in plain language; Frequency; Time in the biological field
SV 48 Skeletal Muscle: Borrelia turicatae 3X
SV 47 Smooth Muscle: Borrelia turicatae 3X
CI 8-1 Diaphragm, Inferior aspect: Borrelia turicatae 3X
HT 6 Myocardium: Borrelia turicatae 3X
CI 4a Muscular Layer of the Arteries: Borrelia turicatae 3X
CI 8 Circulation: Xysmalorium undulatum 4X
CI9 Arteries: Borrelia turicatae 3X; Xysmalobium undulatum 4X; Valeric Acid 3X
CI 8e Thoracic Aorta: Borrelia turicatae 3X; Xysmalobium undulatum 4X
ST 10a Parasympathetic Nervous System: Borrelia turicatae 3X; Xysmalobium undulatum 4X
GB11 Mesencephalon: Borrelia turicatae 3X; Xysmalobium undulatum 4X
BL 35 Sacral Parasympathetic Nerves,Preganglionic Branches: Borrelia turicatae 3X
CI 8d-1 Arterioles and Sympathetic Vasoconstrictive Nerves: Borrelia turicatae 3X
ASSESSMENT
Borrelia turicata: a species of the genus Borrelia, a cause of relapsing fever in Mexico and southwest United States, transmitted by Ornithodoros turicata. The subject had innumerable (a bizillion of them as he says) tick bites including many in the tropical jungle of Mexico.
Xysmalobium undulatum: family Asclepiadaceae, with latex cells that contain triterpenes, alkaloids of indolphenanthroindolizidine and pyridine groups; cardenolides; cyanogenitic glycosides; saponins, tannins, and cycllitols. Used for diarrhea, abdominal cramps and topically for skin sores.
Trease and Evans Pharmacognosy 14th Edition WB Saunders 1989 page 47.
The code for Borrelia has changed to Borrelia turicata and is located at electromagnetic sites associated with muscle and sympathetic and parasympathetic nerves, the myocardium, the arterioles and vasosonstrictive sympathetic nerves and the mesencephalon
RESPONSE
His initial response was a gradual improvement. Only during the winter did his Raynaud’s symptoms get worse, however the atrophic skin ulcers began to heal. Skin tightness remained the same. Sleep disturbance, spaciness, abdominal bloating gastro-esophageal reflux all responded completely. His musculo-skeletal complaints were about the same.
SIX YEAR FOLLOW UP
In an effort to determine his long term response, I called him on the phone. I had not seen him in over 5 years. He said that he was doing well. His skin is not nearly as tight as it used to be and he has minimal joint pain. His skin ulcers have healed but he still has a mild Raynaud phenomenom He has no difficulty swallowing, but has an occasional esophageal reflux. He has a Left Bundle Branch Block and a dilated cardiomyopathy that was diagnosed by an echo-cardiogram and he has traces of pulmonary fibrosis. He uses a treadmill without restriction. His exercise tolerance is improving. Even though his thyroid function does not show any T 3 (levothyroxine) or TSH (Thyroid Stimulating Hormone) abnormality, low doses of thyroid glandular extract have been prescribed for clinical reasons.
When asked about the effectiveness of this technology, he responded,"I was sick with scleroderma for 12 years before I used your method of evaluation and treatment. My health began to improve immediately after I began taking the "drops" (imprinted solutions). From my standpoint this treatment is very effective!"
ASSESSMENT
This is a case of environmentally induced scleroderma.
Conventionally, the following environmental agents have been reported to be associated with scleroderma:
Infectious agents:
Cytomegalovirus (CMV)-may trigger a cascade of events in a genetically susceptible host leading to systemic sclerosis. Genetic factors alone cannot fully explain disease expression.
UpToDate(R) 2008; BMC Musculoskelet Disord 2001;2(1):3. Epub 2001 Jul 31;Nat Med 2000 Oct;6(10):1183-6;
Retroviruses
Proc Natl Acad Sci U S A 1989 Nov;86(21):8492-6
Borrelia burgdorferi
J Eur Acad Dermatol Venereol. 2005 Jan;19(1):93-6 International Journal of Dermatology 31 (11) , 820–820 doi:10.1111/j.1365- 4362.1992; Journal of the American Academy of Dermatology 1993, vol. 29 (1), no2, pp. 190-196 (35 ref.)
Chemical Agents:
Organic solvents-paint removers and paint thinners
J Rheumatol 2004 Dec;31(12):2395-401
Vinyl chloride in the manufacturing process
Lancet 1981 Sep 12;2(8246):567-8
Contaminated rapeseed oil (Canola Oil)
N Engl J Med 1990 Mar 29;322(13):874-81; Ann Intern Med. 1990 Mar1;112(5):344-51; Semin Arthritis Rheum 1990 Jun;19(6):313-28
5-hydroxytryptophan (5-OHTrp)
Semin Arthritis Rheum 1990 Jun;19(6):313-28
4,5-tryptophan dione– a neurotoxin
Biomedical Mass Spectrometry and Functional Proteomics Facility, Mayo Clinic, Rochester, Minnesota, USA
Trichloroethane (TCA), Trichloroethylene (TCE), Toluene, and xylene
Am J Epidemiol 1999 Apr 15;149(8):761-70
Bleomycin. A chemotherapeutic drug
J Rheumatol 1992 Feb;19(2):294-6
Pentazocine
Cocaine
Taxanes-chemotherapeutic drugs
Clin Rheumatol. 2003 Feb;22(1):49-52
SUMMARY OF ENVIRONMENTAL INFLUENCES
There is electromagnetic evidence of environmental contact with:
Spirochetes
B.burgdorferi
B. venezuelensis
B. turicate
Protozoa
Leishmania mexicana mexicana
Helminths
Toxcara mystax (Cat Roundworm)
Virus
Feline Infectious Peritonitis virus
Yeast
Candida rugosa
Insects
Dermanyssus pteronyssinus (house dust mite)
Loxosceles recluse (Brown Recluse Spider)
Snake venom
Agkistrodon contortrix-Copperhead (most likely source of envenomization)
Timeresurus elegans-(less likely source of envenomization)
Vaccines
Influenza Vaccine 1993-99
Swine Flu Vaccine
Immune modulators
Transforming Growth Factor
Beta Glucan
Chemicals
DDT
Tetracaine
Ornidazole
Herbs
Xysmalobium undulatum
KINDS OF ELECTROMAGNETIC INFLUENCES
There are:
7 signals derived from infectious agents
2 signals from insects
2 signals from vaccines
3 signals from chemicals
2 signals affecting cytokine cell to cell regulation
1 herb signal
A total of 17 different non-coherent waves produced destructive interference of information and energy conductance resulting in the clinical state of scleroderma.
CONCLUSION
Electromagnetically imprinted solutions with signals from this subject modulated destructive interference and restored normal conductance. As a result of this modulation, electromagnetic destructive interfering signals were no longer identifiable.
Paralleling the iterative modulation of destructive interference by signal imprinted solutions, the subject’s clinical state improved.
In this case, an electromagnetic model was used to provide effective therapy.
Vincent J. Speckhart MD MD(H)

 Source: Wikipedia, the free encyclopedia
Source: Wikipedia, the free encyclopedia Source: Wikipedia, the free encyclopedia
Source: Wikipedia, the free encyclopedia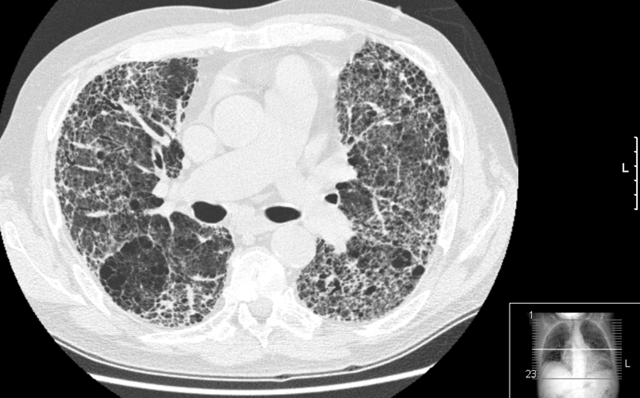
 Source: Tex Heart Inst J. 2002; 29(3): 176–180
Source: Tex Heart Inst J. 2002; 29(3): 176–180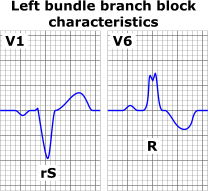
{kind=link}