
Author Archive
Electrodermal Screening and Lyme Disease-trying to go mainstream
Monday, March 3rd, 2008LYME DISEASE, MUSCULOSKELETAL EFFECTS
Monday, March 3rd, 2008History: A 56-year-old female with pain in the left hip and pelvic area, worse with first motion. Pain has been present for 9 months. Other medical problems include migraine headache and Raynaud’s Disease.
Physical Examination: No pain with left hip rotation. The inner aspect of the left iliac wing is painful with deep palpation.
ELECTRO DERMAL PROFILE
FIRST ITERATION
5/9/01
DETECTION SITES/DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Natrum Muriatucum 5X
SV 48 Striated Muscle
Borrelia burgdorferi 3X TIME: 37 years
NV 1b Peripheral and Central Nervous System
Borrelia burgdorferi 3X
NV 1c Spinal Cord and Meninges
Poliomyelitis Virus Type2/Type 3 3x Time: 56 Years
LI 1a-1 Peripheral Motor Nerves of the Upper Extremity T: 137 years Paternal side
HTLV-1 5X
Scrapie 5X Time: 107 years Paternal side
LV 7 Veins of the Legs Isospora belli 3x Time: 74 years Maternal
MIGRAINE HEADACHES
GB 5 Veins of the Head
Isospora belli 3x
RAYNAUD’S DISEASE
SV 91 Auto-immune Process
Plumbum Sulfuricum 3x
CI 9 Arteries
Plumbum Sulfuricum 3x
CI 6 Entire Aorta
Plumbum Sulfuricum 3x
ASSESSMENT
This iteration demonstrates the complex nature of pain. Natrrium Muriaticum is the Pulse-width Equivalent at TW 20, the Hypothalamic Site. This Constitutional State is seen in patients with a low sense of personal esteem who are chronically depressed. The pain in left lower quadrant and hip are associated with Pulse-with Modulated Equivalents for Borrelia burgdorferi at the Skeletal Muscle Site.
The polio signal is identified at the Spinal Cord Site. At this age poliomyelitis has a sensory effect and is associated with pain in the lower extremities.
Scrapie, the frequency associated with HTLV 1, is associated with a Prion neurodegenerative disease. Isospora belli is found in the veins of the leg site and in the veins of the head. In the latter case, protozoa infections of the vein frequently is associated with migraine-like headaches.
Raynaud’s Disease, an autoimmune process, is identified at SV, 91 the Autoimmune Detection Site as well as in the Artery Site and in the site for Entire Aorta. The Pulse-width modulated equivalent at these detection sites is Plumbum Sulfuricum (Lead Sulfate).
Clinical Response: Unchanged.
ELECTRO DERMAL PROFILE
SECOND ITERATION
8/2/01
DETECTION SITES/DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Phosphorus 3X
SV 48 Striated Muscle
Borrelia burgdorferi 32X
NV 1c Spinal Cord and Meninges
Poliomyelitis V. Type2/Type 3 15X
LI 1a-1 Peripheral Motor Nerves of the Upper Extremity
Scrapie 5X
HTLV-1 5X
GB 31 Muscles of the Abdomen and Pelvis
Borrelia burgdorferi 32X
MIGRAINE HEADACHES
LI 18c Ophthalmic Anterior and Middle Cerebral Arteries
Propane 3X
ASSESSMENT
The Hypothalamic Pulse-with Equivalent is Phosphorus, a constitutional sate more consistent with pain intolerance. She is not depressed any longer. The potency for Borrelia, Poliomyelitis, HTLV 1 and Scrapie have all increased.
ELECTRODERMAL PROFILE
THIRD ITERATION
10/11/01
Interval History: Hip pain, migraine headaches signs and symptoms of Raynaud’s Disease are much improved.
DETECTION SITES/DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Phosphorus 12X
SV 48 Striated Muscle
Borrelia burgdorferi 3X,4X,5X,6X, 8X,10X,12X,15,20X,24X,30X
GB31 Muscles of the Abdomen and Pelvis
Borrelia burgdorferi 3X,4X,5X,6X, 8X,10X,12X,15,20X,24X,30X
GB30 Ilium (Pelvic Bone)
Borrelia burgdorferi 3X,4X,5X,6X, 8X,10X,12X,15,20X,24X,30X
NV 1c Spinal Cord and Meninges
Borrelia burgdorferi 3X,4X,5X,6X, 8X,10X,12X,15,20X,24X,30X
ASSESSMET
During this iteration, Borrelia burgdorferi, in multiple potencies, dominated the electro dermal picture.
ELECTRO DERMAL PROFILE
FOURTH ITERATION
2/20/02
Interval History: The patient is completely pain free. “I haven’t felt this good in years”
DETECTION SITES/DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Phosphorus 32 X
Rheumatoid Factor 3X
Platelet Derived Growth Factor 3X
HPV-12 3x
Clinical Outcome: No pain, full range of motion in all joints. Performance Status: Ambulatory and Asymptomatic. (PS 1)
Electro-dermal Outcome: Electromagnetic code for Borrelia burgdorferi is not detected.
LYME BORRELIOSIS Case analysis
Monday, March 3rd, 2008Removing the electromagnetic code for Borrelia burgdorferi
MEDICAL PROFILE
HISTORY: The patient is a 58-year-old male with a history of having had a tick bite in 1984. In the groin, at the site of the tick bite, he developed a classical erythema migrans or “ bull’s-eye” lesion of Borrelia burgdorferi. Skin blisters followed. Heart block, with bradycardia developed in 1989. A pulse sensitive pacemaker was required in 1995.
LABORATORY: At the onset of his disease appropriate titers were obtained for Lyme Borreliosis. Although there was no diagnostic consensus at various laboratories, there was sufficient evidence to recommend treatment with antibiotics.
PHYSICAL EXAMINATION: A chronically ill white male with decreased breath sounds on the right posterior base of the lung, associated with percussion dullness. Heart: regular rhythm with a pacemaker. Skin: Acrodermatitis Chronicum Atrophicans on the arms.
TREATMENT: the use of antibiotics he had a transient response of decreasing fatigue and muscle pain, but this was followed by gradual progression of generalized weakness, muscle cramps, and mental fatigue. Dapsone controlled his skin rash, eruptions and blisters. Severe, nausea, loss of balance and dim vision persisted. He continued to have shortness of breath due to paralysis of the diaphragm on the right side.
ELECTRODEMAL PROFILE
FIRST ITERATION
11/27/01
DETECTION SITE/DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Bug Spray 4X
DIM VISION
OP 7 Macula
Bug Spray 4X
NAUSEA
ST 44c Celiac Plexus
Borrelia burgdorferi 2X
LU 10d Mediastinal Plexus
Bug Spray
LOSS OF BALANCE
TW 17a Cochlea (Inner ear)
Bug Spray 4X
Borrelia burgdorferi 2X
MUSCULAR WEAKNESS
SV 48 Skeletal Muscles
Borrelia burgdorferi 2X
SKIN RASH AND ATROPHY
SK 2 Skin, Upper body
Borrelia burgdorferi 2X
CARDIAC ARRHYTHMIA
HT6 Myocardium
Borrelia burgdorferi 2X
HT 7a (R) Atrio-ventricular Node
Borrelia burgdorferi 2X
HT 7 (L)(R) Conduction Apparatus
Borrelia burgdorferii 2X
NERVOUS SYSTEM
NV 1b Peripheral and Central Nervous System
Borrelia burgdorferi 2X
HEADACHE
GB 5 Veins of the Head
Borellia burgdorferi 2X
ACRODERMATITIS CHRONICUM ATROPHICANS
SK2 Skin of the Upper Body, Arms and Legs
Borrelia burgdorferi 2X
SK1-1 Lymphatics of the Skin
Borrelia burgdorferi 2X
PARALYSIS, RIGHT DIAPHRAGM
BL 17 Right diaphragm, Superior aspect
Borrelia burgdorferi 2X
ASSESSMENT
This case demonstrates a diffuse distribution of Borrelia burgdorferi Pulse-Digital codes The electromagnetic detection sites at which they are found are consistent with the organ and system sites represented by the clinical location of muscle, skin, heart and circulation.
The code for “Bug spray” (otherwise not characterized) has a neurological distribution involving the hypothalamus, cochlea, autonomic nervous systems sites, and the celiac plexus. This suggests that “Bug spray” is a neurotoxic insecticide, either a chlorinated hydrocarbon, or an acetyl cholinesterase inhibitor such as an organophosphate or a carbamate.
ELECTRODERMAL PROFILE
SECOND ITERATION
2/12/02
DETECTION SITE/DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Negative*
* no evidence of a conductance disturbance at the detection site
SV 48 Striated Muscle
Negative
HT 6 Myocardium
Negative
HT 7a Bundle of His (R)(L)
Negative
NV 1b Peripheral and Central Nervous System
Negative
CI 8d Circulation, Main Detection Site
Negative
SK 1-1 Skin Lymphatics
Negative
ST 44c Celiac Plexus
Negative
LU 10d Mediastinal Plexus
Negative
ASSESSMENT
A solution, induced with the code for Borellia burgdorferii, restored conductance. 67 days were required to eliminate non-coherence in the conductance pathway produced by Borrelia burgdorferi.
Clinically, he has no fatigue, no dermatitis, and no muscle weakness. He wants to “get on with life”.
ELECTRODERMAL PROFILE
THIRD ITERATION
4/1/02
DETECTION SITE/DIGITAL CODE IN PLAIN LANGUAGE
Ht 6 Myocardium, Left Side
Babesia ovis 3X
GB 20 Sympathetic Nerve
Candida rugosa 4X
TW 1a Cervical Sympathetic Ganglia
Candida rugosa 4X
SI 1b-1 Small Intestine, Peritoneal Lymphatics
Candida rugosa 4X
DDT 3X
SK 1-1 Skin lymphatics
Borrelia burgdorferi 60X
CI 8-1 Diaphragm, Abdominal , Inferior, Right Side
Borrelia burgdorferi 60X
OP 7 Macula
Bug Spray 8X
GB 19b Eustachian Tube
Borrelia burgdorferi 60X
Bug Spray 8X
GB 17b Cochlea
Borrelia burgdorferi 60X
ASSESSMENT
Approximately seven weeks after the last iteration, Borrelia burgdorferi 60X is detected. The signal is at ‘60X’ suggesting that case is moving toward completion, that is, the non-coherent code has an effect only at a higher frequency.
The code for Bug Spray, postulated to be a neurotoxic insecticide is detected at OP7, the Macula site, and GB 19b, the Eustachian Tube site.
Babesia co-infects the Lyme tick vector and may be a cofactor in his cardiac symptoms as seen at HT 6 the myocardium site
The code for Candida rugosa 4X and other codes for Candida species are frequently associated with Sympathetic Nervous System Sites, suggesting that this code represents a non-coherent signal that is associated with altered conductance at these sites.
Codes for Candida organisms are very frequently associated with the code for the insecticide DDT at small intestine electromagnetic detection sites.
If the code for a Candida organism actually represents the intracellular location of the Candida organism as an endobiont, then the non-coherent signal of DDT may have a disturbing effect on the usually cryptic endobiont allowing it to be detected. The postulate is that the normal intracellular endobionts do not produce a conductance disturbance. They are living in electromagnetic harmony with other cytoplasmic endobionts. There is evidence of both Candida rugosa and DDT at SI 1b-1, the small intestinal peritoneal detection site.
The unresolved understanding of this interaction is whether this only represents an electromagnetic phenomenon or whether this represents an intracellular toxic effect of DDT on the candida endobiont that results in the proliferation of the candida endobiont because of a loss of intracellular homeostasis.
In any event, the DDT/Candida interaction has a distant electromagnetic effect on sympathetic nervous system sites.
ELECTRODERMAL PROFILE
FOURTH ITERATION
10/23/03
DETECTION SITE/DIGITAL CODE IN PLAIN LANGUAGE
Ht 8c Heart, Main Detection Site
Borrelia burgdorferi 800X
Ht 6 Myocardium
Wolframium Metallicum 3X
Ht 8b Endocardium
Borrelia burgdorferi 800X
SK 1-1 Skin Lymphatics
Borrelia burgdorferi 800X
Ht 8e Cardiac Plexus
Wolframium Metallicum 3X (tungsten)
Plumbum Aceticum 3X
Plumbum Metallicum 3X
ST 10a Parasympathetic Nerves
Wolframium Metallicum 3X (tungsten)
Plumbum Aceticum 3X
Plumbum Metallicum 3X
CI 4a Tunica Media, Arteries
Borrelia burgdorferi 800X
ASSESSMENT
The Borrelia code is 800 X at HT 6 the Myocardium site , HT 8b the Endocardium site and CI 4a the Tunica Media of the Arteries Site . The Wolframium (tungsten) code has a parasympathetic nerve electromagnetic location suggesting that the Wolframium signal is associated with the parasympathetic division of the cardiac plexus at the myocardium site. Since the Wolframium signal is located at myocardium site, the Wolframium signal may also affect neuromuscular electromagnetic sites as well. Plumbum (lead) Acetate, and Metallic Lead affect only the parasympathetic site of the cardiac plexus, not the neuromuscular sites.
Lyme Disease-a case report
Monday, March 3rd, 2008LYME BORRELIOSIS, NEUROLOGICAL COMPLICATIONS
History: a 52-year-old white female with Lyme Borelliosis. She gives a history of having had a tick bite on 5/25/85, 11 years previously with classical erythema chronicum migrans rash. There was a gradual onset of cognitive dysfunction, arthritis, fatigue, dyslexia, memory loss, destructive arthritis, and temporomandibular joint pain. She was treated with Doxycycline from 1992 to 1994 with slight temporary improvement of pain.
Physical Examination: The patient presents with a destructive bone lesion of her right shoulder joint, and with right temporomandibular joint pain.
Laboratory: She was serologically positive for Borrelia in 1985.
ELECTRO DERMAL PROFILE
FIRST ITERATION
2/8/96
DETECTION SITE and DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Baryta Carbonicum 4X
LY 1-2 Lymphatics of the Head and Neck
Borrelia burgdorferi 1X
CI 8f Hemo-lymph Nodes
Borrelia burgdorferi 1X
AL 1b Allergy
Borrelia burgdorferi 1X
AR 1b Joints
Borrelia burgdorferi 1X
GV 23-1 Cerebrum
Borrelia burgdorferi 1X
Candida albicans 3X
CI 2 (R) Right Shoulder
Borrelia burgdorferi 1X
AR 3 (R) Temporomandibular Joint
Borrelia burgdorferi 1X
ASSESSMENT
The encrypted signal for Baryta Carbonicum (Barium Carbonate) a homeopathic remedy used for mental weakness and impaired thinking. It is detected at TW 20, a site behind the ear representing the hypothalamus. The functions of the hypothalamus are many, ranging from heat loss to heat conservation, thirst, satiety, water balance, hunger, milk ejection and uterine contraction, circadian rhythms, endocrine activity, emotions, sleep cycles, recent memory, emotions including rage, and autonomic nerve function with both sympathomimetic and parasympathomimetic activity.
Borrelia burgdorferi,a signal for the spirochete causing Lyme disease is detected in sites identified in her clinical history- the cerebrum, right shoulder, right temporomandibular joint.
Candida albicans may be an effect of prior antibiotic treatment for Lyme disease.
ELECTRO DERMAL PROFILE
SECOND ITERATION
4/11/96
DETECTION SITE and DIGITAL CODE IN PLAIN LANGUAGE
CI 8f Hemo-Lymph Nodes
Borrelia burgdorferi 200X
AR 3 (R) Temporomandibular Joint
Borrelia burgdorferi 200X
GV 23-1 Cerebrum
Borrelia burgdorferi 200X
ASSESSMENT
Clinical response: There has been a marked decrease of symptoms. She is able to work and support herself financially.
Electro dermal Response: The potency frequency went from 1X to 200X. The increase in potency is an indication of response.
ELECTRO DERMAL PROFILE
THIRD ITERATION
12/18/98
Interval History: After being lost to follow-up for 2 years and 8 months, she was admitted to a Psychiatric Hospital with a diagnosis of Schizophrenic Psychosis, stupor, prolonged periods of sleep, heart flutter, chest heaviness and myalgia
DETECTION SITE and DIGITAL CODE IN PLAIN LANGUAGE
TW 20 Hypothalamus
Borrelia burgdorferi 10X
Rickettsia Nosode 15X ( Ehrlichia is a tick borne rickettsia)
GB 17 Reticular Formation
Borrelia burgdorferi 10X
Rickettsia Nosode 15X
Amyl Nitrate 3X
Camphor 3X
Cannabis sativa 3X
Paraquat 3X
Strychnine 3X
SCHIZOPHRENIA
GV 23-1 Cerebrum
Borrelia burgdorferi 10X
Rickettsia Nosode 15X
SLEEPINESS/STUPOR
GB 11 Mesencephalon (Sleep/Wake Center)
Borrelia burgdorferi 10X
Rickettsia Nosode 15X
CHEST HEAVINESSHT 8a Lymphatics of the Pericardium and the sub-pericardium
Borrelia burgdorferi 10X
Rickettsia Nosode 15X
MYALGIA
SV 48 Skeletal Muscle
Borrelia burgdorferi 10X
Rickettsia Nosode 15X
ASSESSMENT
Initially there was a response of the digital code for Borrelia burgdorferi going from 1X to 200 X, generally a good sign. In the interval when she was lost to follow up, the potency for borellia decreased to 10 X. This would suggest that there has been a recurrence of her Borreliosis. There has also been a change in the location of the Borrelia signals. They are now located in the central nervous system and are associated with schizophrenia, stupor and sleepiness. The sub pericardium and muscle sites are also affected and are associated with symptoms of the heart and muscles.
Ehrlichia coinfects Ixodes scapularis, the tick vector of Lyme borrelosis. Detection of this signal in multiple sites suggests that there may be a coinfection of Ehrlichiosis.
At GB 17, the detection site for the Reticular Formation, several recreational drug signals have been detected: amyl nitrate (poppers), often used to heighten sexual arousal during drug use; Cannabis sativa (marijuana); paraquat an herbicide used for to destroy marijuana;
strychnine, an illegal stimulant used to adulterate cocaine, heroin, LSD, and other street drugs. GB 17 is a good site to locate psychoactive drugs signals.
ADDENDUM
The patient was lost to follow-up, once again. When contacted in March 2001, she was living in another State and was paralyzed from the waist down due to cancer of the lung invading her spinal cord. I was told that she had an aggressive tumor. Since she previously had lymph node and pericardium signal involvement. One would be led to suspect that she had a small cell undifferentiated carcinoma of the lung since they tend to grow in the midline.
It has been my experience that a signal for cancer is frequently associated with a signal for syphilis, a spirochete. Borrrelia burgdorferi is also a spirochete, leading one to suspect that Borrelia may be a co-factor in the genesis of cancer in this case.
Lyme Disease-Detection sites and signals
Monday, March 3rd, 2008Lyme Borreliosis Electrodermal Detection Sites
Detection of codes for Borrelia species obtained during clinical screening
Sites listed:
- By organs and systems
- Accompanied by electromagnetic detection codes in plain language
Musculoskeletal
- SV 48 Skeletal Muscle
- SV 47 Smooth Muscle
- BL 17 Diaphragm, Superior Aspect
- GB 31 Muscles pf the Abdomen and Pelvis
- GB 30 Pelvic Bone
- KI 23 Intercostal muscles
Heart (Neuromuscular)
- HT 6 Myocardium
- HT 7a (Left) Bundle of His
- HT 7a (Right) Atrio-ventricular node
- HT 7 (Left/Right) Conduction apparatus
- HT 8b Endocardium
- HT 8 Mitral Valve, including the base of the valve
- HT 8a Lymphatics of the pericardium and subpericardium
Nervous System
- NV 1b Main Detection Site, Peripheral and Central Nervous System
- ST1 Degeneration in the Head
- GV 23-1 Cerebrum
- GB 17 Reticular Formation
- GB 4 Thalamus
- TW 20 Hypothalamus
- GB 7 Mesencephalon
- GB 11 Diencephalon (Sleep/Wake Center)
- BL 8a Inferior Colliculus
- NV 1c Spinal Cord and Meninges
- ST 44c Celiac Plexus (Autonomic)
- TW 13 Autonomic Innervation of the Skeletal Muscles
Skin
- SK 1-3 Skin, Main Detection Site
- SK 1-1 Lymphatics
- SK 1 Skin, Lower Extremity
- SK 3 Skin, Head and Scalp
Joints
- AR 1c Synovial Membranes of the Joints
- CI 2 Shoulder Joint
- AR 3 Temporomandibular Joint
- SV 72 Sacro-iliac Joint
- LI 16 Finger Joint
- GB 29 Hip Joint
- SV 75 Cervical Vertebra
- SV 73 Thoracic Spine
Circulation
- CI 8d Circulation, Main Detection Site
- GB 5 Veins of the Head
- CI 8f Hemo-Lymph Nodes
- LY 1 Palatine and Deep Cervical Lymph nodes
- NV 1d Microcirculation of the Brain
- CI 4a Tunica Mediia of the Arterial Wall
- CI 8e Thoracic Aorta
- CI 8c Abdominal Aorta
- CI 5 Brachial Artety
- CI 7 Coronary Artery
- CI 8b-1 Capillaries and Venules
Gastrointestinal
- SP 1a (Right) Pancreas, Main Detection Site
- SP 4 (Right) Pancreatic Lipase
- GB 44 (Left) Common Hepatic Duct
- ST 45 (Left) Body of the Stomach
Digitalized Borrelia species in the computer
Worldwide, there are 38 known species
Borrelia:gram-negative, anaerobic, parasitic spirochete, living on mucous membranes, the cause of relapsing fever in humans and animals.
Borrelia berbera=B. recurrentis
Borrelia burgdorferi: agent for Lyme diaesae
Borrelia carteri=B. recurrentis
Borrelia caucasica: agent of relapsing fever in the Caucasus, transmitted by the tick Ornithodoros verrucosus from a reservoir of infection in field mice
Borrelia duttonii: agent of endemic relapsing fever in Central and South Africa, carried by the tick Ornithodoros moubata, transmitted from human to human in saliva
Borrelia hermsii: agent of endemic relapsing fever in western North America, transmitted by the tick Ornithodoros hermsii, which is transported by chipmunks and tree squirrels
Borrelia hispanica: the etiologic agent of endemic relapsing fever in the Iberian peninsula and Northwest Africa, transmitted by the large tick Ornithodoros erraticus, which lives on rodents, reptiles, and amphibian
Borrelia kochii=B. duttoni
Borrelia morganii not listed, may be Morganella morganii
Borrelia novyi =B. duttoni
Borrelia parkeri:an etiologic agent of endemic relapsing fever in the western United States. Burrowing rodents, such as ground squirrels, carry the tick vector, Ornithodoros parkeri, which transmits the organism in its bite
Borrelia persica: an etiologic agent of endemic relapsing fever in Asia and Africa. The organism is transmitted in the bite of the tick vector Ornithodoros tholozani, which is carried by rodents living in caves, stables, and burrows.
Borrelia recurrentis: causative agent of worldwide epidemic louseborne relapsing fever, transmitted by the human body louse, Pediculus humanus. The organism is spread by rubbing infected hemolymph of lice into the skin, as in scratching. The organism produces successive antigenic mutants that cause the clinical relapses. Called also B. berbera, B. carteri, B. novyi, and B. obermeyeri.
Borrelia tillae no currently listed taxonomy
Borrelia turicatae: an etiologic agent of endemic relapsing fever in southwestern United States and Mexico. The organism is transmitted by the bite of the tick Ornithodoros turicata, which is carried by rodents and reptiles
Borrelia venezuelensis:etiologic agent of relapsing fever in Central and South America, transmitted by the tick Ornithodoros rudis, which is carried by monkeys and rodents=B. neotropicalis
Borrelia vincentii=Treponema vincentii. A spirochete associated with acute necrotizing ulcerative gingivia
Comment
In my clinical trials, Borrelia species had the most widespread distribution of bacterial signals. Treponema was detected the largest number of times.
Clinically, borreliosis signal recognition is a common finding when using electrodermal detection technology.
Correction of the borrelia codes is effectively accomplished by using signal induced solutions.
Top of Form
Bottom of Form
Lyme Disease Review
Monday, March 3rd, 2008Lyme Borreliosis
Medical Profile
Borrelia burgdorferi is a fastidious microaerophilic spirochete, the causative bacterium for Lyme borreliosis. Three groups of Borrelia organisms have been cultured. They are collectively called Borrelia burgdorferi sensu lato. Group 1 (B. burgdorferi sensu stricta) is found in North America; Group 2 (B.garini) and Group 3 (B. afzeldi) are found in Europe and Asia.
The principle vectors are the ticks Ixodes scapularis in the Northeast, Ixodes pacificus in California and Oregon, Ixodes ricinus in Russia, China and Japan. I. Scapularis may transmit Babesia, Ehrlichia and Rickettsia.
Infectivity of the tick is carried out by the tiny nymph stage in the early summer months. The white-footed mouse is the host for the larva-nymph stage. The white tailed deer, not involved in the life cycle of the spirochete, is the preferred host for the adult Ixodes scapularis tick. Adult ticks occasionally transmit the spirochete to humans in the fall of the year.
Clinical manifestations: Stage 1, localized infection: After an incubation period 3 to 32 days, the initial lesion, erythema migrans (EM) is found at the site of the tick bite. This is an annular lesion with a red border and a central cleared area. Twenty five percent of patients are negative for this reacton. Stage 2, disseminated infection: After infection hematogenous spread with flu-like symptoms develop. Patients complain of headache, fever, chills, arthralgia, myalgia, malaise and fatigue. Cough and sore throat are prominent. Peripheral and central nervous system symptoms may develop after several weeks. Variable cardiac events may occur ranging from first degree A-V block of Wenckebach to complete heart block. Even myocarditis, pericarditis, and left ventricular dysfunction can occur. Musculoskeletal pain is common. Joint pain is usually without swelling. Stage 3, chronic infection: At this stage the joints are most commonly affected, especially the larger joints. Neurological changes, with memory loss, mood changes, and sleep disturbances are the most common symptoms. Severe myelitis (inflammation of the spinal cord) may also occur. A chronic course of neuro-borreliosis resembles the latent effects of another spirochete infection, tertiary neuro-syphilis.
The skin demonstrates acrodermatitis chronicum atrophicans.1,2
1. Steele A., Lyme borreliosis, Harrison’s Principles of Internal Medicine 15th edition, p1061-1064, McGraw-Hill, New York 2001
2. Mégard, F., van Loon F., & Thijens, S., Lyme disease, Infectious Diseases, p 8.19.9-11, Mosby, London, 1999
3. UpToDate © 2007
The Complex Human Biological System
Monday, February 25th, 2008This study focuses on the electromagnetic characteristics of a biological system. As a part of a very complex and dynamic biological system, electromagnetism interacts with every part of the system.
Chart 1 is my perspective of some components of the human biological system. It is based on the author’s 40 years experience as a general internist, a flight surgeon, a foreign Christian medical missionary, a medical oncologist and researcher, a founder of a hospice for the terminally ill, a licensed homeopathic physician and an electrodermal researcher.
In this overview I hope to create awareness that there are a number of influences modifying biological conductance that we, in the scientific community, are reluctant to consider because they are not able to be measured and therefore not able to be subjected to statistical validation. This reluctance applies especially to things of the ‘spirit’; less so to matters of the ‘soul’ but it does not mean that ‘spirit’ and ‘soul’ are not relevant to the healing process. Nor is ‘God’ irrelevant for that matter. It is just that in the current scientific paradigm, faith and revelation are too subjective to be considered for analysis. If these areas of concern need to be considered for total healing, than there has to be a paradigm shift in our approach of how to bring about healing.
An Overview of the Complex Human Biological System
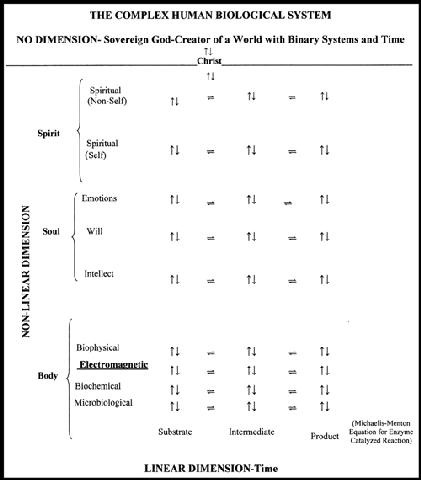
A line divides the chart into two parts. The upper part refers to the realm of God; the lower part refers to the created realm of space-time.
Since this is a study of electromagnetic changes over time, the chart is structured to reflect the dimensions of the system that can be measured electronically.
The linear dimension of time is shown on the abscissa.
The nonlinear dimensions of body, soul and spirit are shown on the ordinate.
Outside of space-time there is a state that cannot be measured because it is infinite. It is limitless and so it has no outside boundary to measure and, therefore, has no dimension. It is the realm in which God exists. Our cortex functions best in three dimensional space and time, so we know some of the attributes of God by things that are created such a beauty, power, strength and majesty but there are attributes of God that cannot be reasoned to or experienced. These can only be known through revelation.
There are two sources of knowledge: experience and revelation. Experience is knowledge obtained by observing events in space-time. Revelation is knowledge that comes from outside of oneself and is of human or divine origin.
Human revelation is knowledge communicated through our senses from the outside but confined to space-time such as a lecture, a conversation, seeing a beautiful sunrise or feeling a warm breeze. Divine revelation is knowledge communicated to creation from God by inspiration or direct revelation. With divine revelation certain characteristics of God can be known. For this we must rely on the inspired writings given to scriptural writers such as Moses in Genesis 1:1. “In the beginning God created the heavens and the earth”. Since He created space-time dimensions He must have existed before them in a non-dimensional state and must not have been dependent on creation for His existence (sovereignty). Words themselves limit the true nature of God by assigning to Him attributes from the things created in space-time and ascribed to Him as characteristics that we understand from the things he formed, even ascribing to Him a sexual nature. Before His revelation to Moses on Mount Sinai he was known to the Patriarchs as El Shadai, the Nurturing Mother. After giving the Law on Mount Sinai he became known as Yahweh, the Law Giving Father. Both a male and a female nature of God had been revealed to Moses and the Patriarchs.
Below the realm of the Sovereign is the created realm of space-time separated by a broken line in which the word “Christ” is inserted, representing His duel nature as God and Man, as mediator between the Sovereign and the created realms.
On the abscissa there are three columns going from A to B to C. Each column has arrows pointing in both directions is in equilibrium with the other. Time is the only dimension in the three columns; therefore, the abscissa describes a linear dimension. Arrows point in two directions horizontally and vertical. Consequently, all other dimensions are influenced by time. This serves as a basis for using a process of iteration to observe a clinical outcome. Changes in biological events take time. I’ve used the Michaelis-Menton equation of enzyme catalyzed reaction to point out that biochemical reactions occur over time- from substrate to intermediate to product.
The ordinate demonstrates the qualities that are distinct from each other: body, soul and spirit. These qualities are nonlinear.
In the body realm there are methods of measuring and describing microbes, biochemical reactions, electromagnetic wave and other biophysical effects such as temperature and pressure. All of the above states can be quantified.
The soul realm consists of the intellect (mind), will and emotions. There are scientific documents that allow for measurements of each of these entities. The IQ test is one example.
The spirit realm is difficult to characterize or measure. Broadly speaking, the spirit that exists within man can be separated from those spirits that exist outside of man. Some have described man as having a spiritual and a carnal nature, the spiritual nature being eternal, the carnal nature ending in death.
At an even higher level there are spiritual forces outside oneself. These are of two classes: Angels, messengers of God dispensing blessings, and Demons, agents in opposition to the purposes and plans of God.
Arrows denoting equilibrium have been placed between all the linear and nonlinear dimensions of the chart in order to show that a disturbance at any point in the chart affects biological conductance in every other part.
This chart is meant to convey the concept that the human, living, dynamic, multidimensional biological system is very complex and that in establishing normal conductance, all dimensions of man must be considered, even at level of spirit or soul.
This complexity demonstrates the difficulty of developing a method of statistical analysis. The possibility of stratifying the same dimensions in two identical populations over time is extremely difficult if not impossible.
One is forced to observe outcomes. Evaluation in this study is based on modifying the electrodermal profile by using electromagnetic codes that restore conductance and by the parallel observation of clinical outcomes when conductance is restored.
The Boolean (binary) system of opposites, the purest form of communication, is present throughout creation: yes/no, on/off, and/or, neither/nor, up/down, right/left, in/out, one/zero, good/ bad, light/dark, life/death. The Boolean system is demonstrated in this chart by arrows going in opposite directions.
The arrows demonstrate the interconnection of all dimensions of creation.
Even the I/O of the computer can interface with this system and is the technical basis for this study.
This chart demonstrates that nothing in space-time is independent of a Sovereign God through Christ.
Process of Iteration
Saturday, February 16th, 2008The following discussion continues to build a foundation by which the reader can increase his understanding of the eletro-dermal screening process. Exposure to outside influences (interferences) impacts the body systems. In order to address these interferences, they must be detected, identified, and measured. This paper provides an overview of the evolutionary, methodical approach to develop a standard process of screening.
Process of Iteration
When I first began to research electrodermal detection, I developed a guide to locate electromagnetic skin sites according to organs and systems. I grouped the detection sites by organs and systems because most health professionals are taught to make a diagnosis using this approach.
The following list is an overview of organ and system detection sites. Each heading has many subdivisions that will be commented upon later as this journal progresses.
Organ and System Detection Sites
Allergies
Arteries
Blood
Breast
Connective Tissue
Degeneration
Ear
Endocrine
Eye
Fat Tissue
Gallbladder and Bile Ducts
Gastrointestinal Tract
Heart
Hormones
Immune System
Joints
Liver
Lymphatic System
Mucous Membranes
Musculoskeletal System
Nasopharynx
Nervous System
Odontons (Teeth)
Pancreas
Respiratory System
Skin
Spleen
Urogenital System
Veins
Palmar Arrays
Subsets of the detection sites
Each detection site has:
A name in plain language;
An electromagnetic site designation
A page for site location (bold/italic) found in the Atlas of my book, An Electrodermal Analysis of Biological Conductance
Large Intestine
Main Detection Site: LI 1b 5, 6
Greater Omentum: LI 3a 5, 6
Omental Bursa: LV 10 30
Cecum – LI 4 (R) 5
Lymph Vessels: LI 1-1 (R) 5
Superior Mesenteric (Autonomic) Plexus: SI 1a (R) 21
Smooth Muscles: LI 7 7
Appendix-Ileocecal Lymph Nodes: LI 4a (R) 5
Ascending Colon: LI 3 (R); LU5 5; 4
Lymphphatics , Cecum and Right Colon: LI 1-1 5
Superior Mesenteric (Autonomic) Plexus: SI 1a (R) 21
Peritoneum: LI 1c (R) 5
Peritoneal Lymph Vessels: LI 1b-1 (R) 5
Hepatic Flexure: LI 2 (R) 5
Superior Mesenteric (Autonomic) Plexus: SI 1a (R) 21
Sympathetic Nerve Hepatic Flexure of the Right Colon: LU 4 (R) 4
Transverse Colon, Right Side: LI 1 (R) 5
Superior Mesenteric (Autonomic) Plexus: SI 1a (R) 5
Transverse Colon, Left Side: LI 4 (L) 6
Inferior Mesenteric (Autonomic) Plexus: SI 1a (L) 21
Splenic Flexure: LI 3 (L); LU 5 (L) 6; 22
Inferior Mesenteric (Autonomic) Plexus: SI 1a (L) 21
Descending Colon: LI 2 (L) 6
Inferior Mesenteric (Autonomic) Plexus: SI 1a (L) 21
Descending Colon, Sympathetic Nerve: LU 4 (L) 4
Inferior Mesenteric Lymph Nodes: LI 4 -1 (L) 6
Sigmoid Colon: LI 1 (L) 6
Lymph Vessels: LI 1-1 (L) 6
Inferior Mesenteric (Autonomic) Plexus: SI 1a (L) 21
Inferior Mesenteric Lymph Nodes: LI 4 -1 (L) 6
Mesocolic Lymph Nodes: LI 4a (L) 6
Recto-Sigmoid Mucosa (L-3): GV 3a 61
Anus
Anal Canal: KI 5 50
Anal Sphincter: KI 4a; BL 30 50; 54
Rectum—KI 6 50
Medial and inferior (Autonomic) Plexus: KI 4 50
Venous (Hemorrhoidal) Plexus: KI 5a 50
Mucosa: SV 22 63
Recto-vesical/Recto-uterine (Douglas) Pouch: KI 6c 50
In my text An Electrodermal Analysis of Biological Conductance made an atlas demonstrating the topographical locations of these electromagnetic sites.
The graphic below is an example of one of the atlas pages.
It’s all information-codes, waves or signals
In 1996 I developed a protocol for recognizing clinical relevant non – coherent waves. The database that resulted identified the most frequent detection sites as well as the most frequent non-coherent encoded signals at those sites.
I then arranged the non-coherent codes by using plain language. I gave a short scientific description for each entry and I listed them alphabetically and by category in a glossary to be clinically useful. Were the signals related to a virus, bacteria, a fungus, toxic metal or toxic chemicals, etc.? It was my desire to make electrodermal detection a practical tool for use in the medical system as it is practiced today. Below is a list of these categories from my data.
Plain Language description of signals
Based on an analysis of 1310 files from 600 subjects from 1/8/93 to 3/8/98
Encoded Groups Number of Codes in Each Group
1. Tissue Nosodes 123
2. Bacteria 113
3. Chemicals/Drugs 112
4. Viruses 78
5. Fungi 69
6. Protozoa 53
7. Metals 46
8. Helminths 37
9. Homeopathics 30
10. Constitutionals 21
11. Cytokines 19
12. Dental 18
13. Miasms 15
14. Insects 10
15. Plants 5
16. Imponderables 5
17. Animal 4
18. Foods 3
19. Prions 3
20. Metabolites 2
Total 676
The above listing represents the broad categories of encoded non-coherent waves. There are 676 total codes in this list. Since then many more have been added.
In this section I will show how to select these waves by the process of iteration.
Iteration is defined by Merriam-Webster’s Collegiate Dictionary 10th edition as “a repetition of a sequence of operations that yields results successfully closer to the results desired”.
Recovery from illness is a biological process that takes place in a sequential fashion over time. For example, after a laceration, a clot must be formed first, followed by fibroblastic infiltration and subsequently by scar tissue formation.
In the homeopathic school of thought, Herring’s Law of Cure states that healing takes place from the inside out, from the top-down and from the acute to chronic. The analogy of peeling off the layers of an onion is often used.
Reckoning
(Merriam – Webster’s Collegiate Dictionary 10th edition 1993)
Definition: To accept something as certain; to judge
It has been found by reckoning, that electromagnetic elimination of non-coherent waves are associated with improvement in clinical conditions. The process of reckoning occurs in a sequential fashion over time.
Before we discuss the process of eliminating non coherent waves we should try to resolve the difference between a diagnosis and electrodermal signal detection
A diagnosis carries with it a precise description:
Diagnosis:
(Merriam – Webster’s Collegiate Dictionary 10th edition 1993)
1a. the art or acts of identifying a disease from its signs and symptoms
1b. the decision reached by diagnosis
2. a concise technical description of a taxon (classification).
3a. investigation or analysis of the cause or nature of a condition, situation, or problem
3b. a statement or conclusion from such an analysis
Diagnosis
(Blacks Law Dictionary, Abridged 6th edition, West Publishing Company St. Paul MN 1991)
1. A medical term, meaning the discovery of the source of a patient’s illness or a determination of the nature of his disease, from a study of its symptoms.
2. The art or act of recognizing the presence of disease from its symptoms and deciding as to its character. The decision reached for determination of type or condition through case or specimen study or conclusion arrived at through critical perception or scrutiny.
A “clinical diagnosis” is one made from the study of the symptoms only.
A “physical diagnosis” is one made by means of physical examination such as palpation and inspection.
A “ pathological diagnosis” is made by an interpretation of a pathological specimen” by a pathologist.
My definition of diagnosis is:
A consensus medical profile based on an analysis of a case history, a physical examination and an interpretation of laboratory and other technical studies for the purpose of treatment by those trained in this paradigm.
Electrodermal detection or Electrodermal Screening
Is a screening devise, in the nature of a laboratory test for gathering electromagnetic information. By itself it does not provide some of the information needed to establish a diagnosis, such as, the need for signs or symptoms or other usual laboratory data. Electrodermal detection cannot be used to make a diagnosis but the information provided can support a diagnosis. It is different from other laboratory tests in that it is an electromagnetic recognition devise, and does not provide chemical or biological information. In that sense it stands alone as a model for providing information.
The purpose of the process of iteration is, first of all, to establish an electromagnetic profile and then modify this profile in order to re-establish normal conductance.
Method of developing an electromagnetic profile
Every electromagnetic detection site on the surface of the skin represents an electromagnetic site of origin for a conducting or non-conducting electromagnetic signal.
Not all detection sites are in a convenient location for direct testing nor are all sites sufficiently sensitive to give consistent skin resistance readings by testing from that site.
When a current of injury such a pinprick, or focal pressure or electrical charge from the test probe, is applied at an inconvenient or insensitive detection site, there is amplification of the signal at that site. The injury stimulus makes the signal easier to be detected at the Main Detection Site thus making it the preferred site for applying the detecting probe.
Another way to highlight a detection site is for the one being tested to touch the detection site with the index finger of the hand holding the negative electrode; (the probe is the positive electrode.) The contacted site may then be tested at the Main Detection Site. This technique is especially useful for testing sites in “socially sensitive” areas.
Problems with detection sites:
Some detection sites are not conveniently located.
Some are on the back, others in the breast area, on the buttocks or in the groin.
Many of the inconvenient sites are also too weak to give good detection signals.
Main Detection Sites
Are located in the periphery of the fingers and toes near normal bone anatomical sites
They are easy to reach and easy to manipulate.
Are important because they represent electromagnetic events along the entire detection array especially those sites that have been highlighted or stimulated
Signals from any skin detection sites can be transferred to the Main Detection Sites of that array by a simple two-step maneuver:
1. Touch (stimulate) the desired detection site.
2. Test at the Main Detection Site of that Detection Array and observe the ohmmeter response.
Example:
If you want to determine a code at GB 5-Veins of the Head:
1. Stimulate GB 5 with the probe tip
2. Apply the probe at GB 43b, the Main Detection Site for the Gallbladder Array and observe for changes in skin resistance.
A changes at GB 43b actually reflects a changes at GB 5
Speckhart’s Protocol for Electromagnetic Profile Development
Purpose of the Protocol: To rapidly survey detection sites and codes.
The following is a list of some the more frequently used detection sites.
H-H Hand to Hand
Main Detection Sites
LY 1-2 Head and Neck
LU 10c Lungs
LI 1b Large Intestine
NV 1b Peripheral and Central Nervous System
CI 8d Circulation (Arteries, Veins, Lymphatics)
AL 1b Allergies
OR 1b Cellular Metabolism
TW 1b Endocrine System
HT 8c Heart
SI 1b Small Intestine
Sp 1a (R) Pancreas
Sp 1a (L) Spleen
AR 1b Joints
ST 44b Stomach
FI 1b Connective Tissue
SK 1-3 Skin
FA 1b Fatty Tissue
GB 43b Gallbladder and Bile Ducts
KI 1-3 Kidney
BL 66b Urinary Bladder and Urogenital Organs
Other Important Detection Sites
TW 20 Hypothalamus
OR 1-1 Lymphatics of Organ Degeneration
LY 3 Nose and Paranasal Sinuses
LY 2 Jaw and Teeth
SV 48 Striated Muscle
GB 17 Reticular Formation
SV 61 Eosinophils
GB 5 Veins of the Head
SV 46 Periosteum
AR 1c Synovial Membranes
NV 1c Spinal Cord and Meninges
The Process of Healing
Saturday, January 5th, 2008When we think of healing we usually think of wound healing. In this type of healing, there is a complex sequence of events that occur immediately after the injury, all carefully orchestrated by a cascade of biochemical reactions that end in repair of the injured site.
These phases are:
Inflammatory phase:
Formation of a cascade of clotting factor to stop bleeding
Platelets aggregation forming a mass (plug) by sticking to one another
Vasoconstriction-an initial narrowing of blood vessels to stop bleeding
A subsequent vasodilatation, to increase healing factors into the wound
Polymorphonuclear neutrophil influx (White blood cells) which:
Help to digest debris and bacteria
Kill bacteria by releasing oxygen free radicals
Clean the wound by secreting enzymes that degrade damaged tissue Undergo apoptosis-a process of programmed cell death
Macrophages (immune white cell) which:
Engulf and degrade white blood cells
Stimulate cells that cover the wound with skin
Create granulation tissue, connective tissue and tiny blood vessel on the surfaces of a wound during the healing process
Lay down extracellular matrix-a gel-like complex sugar that binds cells together
Proliferative phase (a phase of rapid production of new cells and substances)
Angiogenesis-the making of new blood vessels needed for healing
Fibrin and fibronectin-cross-linked fibrous strands to trap proteins and particles
Deposition of collagen-the main protein of connective tissue
Formation of fibrous connective tissue
Epithelialization phase
Final stage of healing with formation of skin over the wound
Contraction
Shortening of the scar
You may pass off your injury with the comment “Oh, it’s just a cut” but you can see from the above outline that the process of healing is incredibly dynamic and complex.
Repair of other types of tissues like bone, nerve, tendon, muscle etc. require similar complex interactions. Viruses, fungi, bacteria and parasitic infections can cause disease and have to be controlled to maintain a state of health as do chemical toxins and toxic metals. There are unique processes in place for healing in each of these areas.
I want to emphasize the word process. That is, there is a beginning, an intermediate phase and an ending. Healing events take place over time, not instantaneously.
As noted above the process of healing can be influenced by a variety of factors including infections, nutritional and immune deficiencies, age, chemicals, toxic metals, heat, coldness or organ failure. And that is just at the physical level.
Influences at the level of the soul, consisting of the intellect, the will and the emotions, may also influence healing, suggesting an interrelationship between these two levels of the body’s design.
Lastly, there is the influence of the spirit, not conventionally included as being important in the healing process, when, in fact, it may be one of the key elements in this process.
Since we are spirit, soul and body, true healing can only take place with harmony at all three levels of organization. I will expand on this topic with a discussion the complexity of the human living system in a future journal entry.
Our discussion will deal with the physical level first. We will show how computer generated electromagnetic signals alter skin resistance and how these electromagnetic altering signals initiate the healing process and sequentially track the healing process until it is completed. It is a wonderfully organized and integrated process.
Scientific discovery yields information that varies with the model that is being used. A model is a representation of “reality” based on tools and observations used in conducting such a study.
A surgeon, studying wound healing, may use a model based on wound closure with sutures, clips or bandages.
A forensic pathologist may use a model based on the kind of wound, whether it is a laceration, a puncture wound by a knife or bullet.
A microbiologist could use a model based on infectious processes that may affect wound healing.
A molecular biologist may want to use a biophysical or biochemical model to determine the sequence of events taking place during the wound healing process.
Our model is a biophysical model in which we compare information that is radiating through a biological system with information stored in a computer system. As an example, detection of an electromagnetic signal representing a bacterium in a skin wound would be useful in establishing an association with a wound infection.
There are two models for electrodermal detection (see my posting: “Treatment Priorities in Electrodermal Testing”).
In the first model, all of the signals stored in the computer are compared with all of the abnormal signals in the biological system.
This model is a general search for abnormal signals
Is not specific for detecting the sites of abnormal signals
It cannot be used to construct an electromagnetic profile for a clinical condition
Does not lend itself to be used in detailed sequential analysis
Disregards priorities set by the biological system
Your body is aware of sites of injury. Just hit your finger with a hammer and it will not take you very long to discover the priority your body has set for pain in the nail you just injured.
The electrodermal system will detect abnormal signals at sites of injury as well.
The second model focuses on biological specificity.
It is the method we have chosen
It is a more targeted method of analysis, one based on the sequential analysis of specific sites over time
This model is an iterative or a repetitive analysis at the same site
It is directed at altering abnormal signals until they can no longer be detected
The relationship between electromagnetic profiles and medical profiles (diagnosis) can be made easily
For example, you can identify the signals that are associated with rheumatoid arthritis or cancer or many other conditions and you can observe the electromagnetic changes that take place during the healing process
Changes can be tabulated for statistical review
Both of these models are electromagnetic in character. For practical purposes we can disregard the magnetic aspect of the signal and concentrate our discussion on its electrical characteristics only. In order to do this, an understanding of the role of physics in biology is necessary. This will be the subject of our next journal entry.
Textbook of Pediatric Emergency Procedures, Henretig, F, King, C (Eds), Williams and Wilkins, Baltimore 1997. p.1141.
Midwood K.S., Williams L.V., and Schwarzbauer J.E. 2004. Tissue repair and the dynamics of the extracellular matrix. The International Journal of Biochemistry & Cell Biology, 36(6): 1031-1037.
Stadelmann W.K., Digenis A.G. and Tobin G.R. 1998. Physiology and healing dynamics of chronic cutaneous wounds. The American Journal of Surgery, 176(2) 26S-38S.
Vincent J. Speckhart MD
Treatment Priorities in Electrodermal Testing
Monday, December 17th, 2007
Over the years of practicing medicine, I have found that the patient can tell you what is really wrong most of the time, when you actively listen. If needed, the physician may add a few diagnostic studies to determine the medical or surgical specificity of the problem, but it is the patient who sets the priorities based on his awareness of what is going on internally. In history taking we call the patients understanding a ‘Chief Complaint’. We usually follow this by a ‘Review of Systems’ to determine the influence this complaint has on body organs and systems or to see if there are independent conditions unassociated with the chief complaint. Seidel Henry M. Mosby’s Guide to physical examination (St. Louis: Mosby-Year Book Inc. 1995
Homeopathic physicians, on the other hand, want to know the ‘totality of symptoms’ in order to establish a priority for prescribing a remedy. It is the client who provides the information. It is his symptoms that establish the priority for treating. Boericke, William, Homeopathic Materia Medica, 9th Edition, (Santa Rosa: Boericke and Taffel Publishers; The Homeopathic Pharmacopoeia of the United States, 8th Edition Volume I (American Institute of Homeopathy
1979)
In acupuncture theory, energy flows in channels beneath the skin. These channels represent energy flowing from certain organs or systems to the skin. Symptoms may be modified by inserting a needle at sites along an energy channel. Selection of a specific site for treatment is based the acupuncturist’s understanding of signs or symptoms even though the individual is unaware of the acupuncture meridian system through which the energy flows. It is the individual’s awarenesss of internal events that sets the priority for the site selection of acupuncture needle insertion. Chen, Kuo-Gen, Electrical Properties of Meridians (IEEE Engineering in Medicine and Biology Magazine pp
58-63, Volume 15, Number 3 1996)
When looked upon from an electrodermal perspective, energy flows in lines similar to acupuncture channels. Energy flows in pulsed patterns that convey specific bits of information. As in acupuncture, information originates in an organ or system and is conducted to a specific site on the skin without the individual’s awareness of the information being conducted. Alteration of electromagnetic conductance in the organ or system is not only associated with signs and symptoms but is also associated with information being conducted through electromagnetic pathways to specific locations on the skin. The patient is aware of the signs and symptoms but is unaware of the information being conducted nor is he aware of the electromagnetic pathway through which they are being conducted. The individual’s energy flow pattern sets the priority for the sites to be tested. An Electrodermal Analysis of Biological Conductance (Biological Conductance Inc. Virginia Beach VA 2004
Once the initial conductance abnormality is corrected, retesting will demonstrate priorities for the next set of tests. This process (iterative analysis) is continued until the case is completed, that is, there is no longer a conductance abnormality. There may be more than one set of priorities in an examination. Conductance disturbances may be corrected in each of these at the same time.
The advantage of this type of analysis is that the process is patient directed and not ‘machine’ directed. Clinical improvement and electromagnetic changes are able be observed at the same time. The goal for electromagnetic intervention is to obtain a favorable clinical outcome, not to eliminate of all abnormal wave forms.
Until we have a clear understanding of the interrelationship of normal and abnormal waves, both before and after intervention, we should try to detect the fewest number of signals in the conductance pathway that are needed to bring about a favorable clinical outcome. We should try to reduce the number of destructive waves in the conductance pathway that could possibly be introduced by random induction of signals.
In my judgment, iterative analysis is the best way to accomplish this objective and is the best way to develop a scientific format for statistical analysis and data recording.
Vincent J. Speckhart MD, MD(H)